

You’ve decided to address your low testosterone—a smart move that could transform your energy, mood, muscle mass, and libido. But now you’re facing a critical decision: enclomiphene or testosterone replacement therapy (TRT)?
Both can raise your testosterone levels. Both have devoted supporters. But they work through completely different mechanisms, carry different risks, and suit different men at different life stages. And here’s what separates MOPE Clinic from every other provider: we don’t guess. We test. We compare your actual labs to your goals, and then we prescribe.
This isn’t marketing language. It’s the difference between a real medical decision and a shot in the dark.
Let’s break down the science, the pros, the cons, and why one might be perfect for you while the other could be a mistake.
The Problem
You’re dealing with low testosterone. You feel it—maybe it’s afternoon fatigue that won’t quit, or muscles that don’t respond like they used to, or a libido that’s lost its spark. You’ve read that testosterone can help. But when you start researching treatments, you find conflicting advice, online clinics promising quick fixes, and a confusing landscape of options.
The truth: most men never get a real comparison. Meanwhile, they stumble onto one option, assume it’s the only path, and make a decision without understanding the full picture.
Ultimately, that’s how mistakes happen.
Why It Happens
The internet is flooded with information—however most of it biased or incomplete.
Meanwhile, many online clinics push TRT because it’s profitable and creates ongoing prescriptions. Additionally, supplement companies promote enclomiphene because it’s newer and less regulated. Forums are filled with anecdotal stories that don’t apply to your body or your situation. And most urgent care clinics or general practitioners don’t have time (or expertise) to properly explain the trade-offs.
So men choose based on:
- What they read first
- What sounds safer (without understanding what that means)
- What’s cheaper
- What seems faster
- What some influencer recommends
Ultimately, none of these are good reasons to choose a hormone treatment.
Why Normal Methods Fail
The typical approach to choosing between enclomiphene and TRT looks like this:
1. Self-diagnosis: You read an article, identify with some symptoms, and ultimately assume low testosterone is your problem.
2. Incomplete labs: You get a single testosterone level checked (often just total testosterone, not free testosterone, SHBG, estradiol, or LH).
3. One-sided information: You talk to a provider who specializes in only one treatment and, surprise, they recommend it.
4. No baseline comparison: You never compare your individual lab values, age, health history, fertility plans, or lifestyle to what each treatment actually does.
5. No monitoring plan: You start one option, maybe don’t feel results in 2 weeks (even though hormonal changes take 4-8 weeks), and because of that you switch.
The result: men on the wrong treatment, wrong dose, or wrong timing. Some men experience unnecessary side effects. Others lose fertility they could have preserved. Additionally, many also spend money on treatments they never actually needed.
What Actually Works
A real medical decision requires five things:
1. Comprehensive baseline labs. Not a single testosterone number—a full hormone panel: total testosterone, free testosterone, SHBG, estradiol, LH, FSH, prolactin, and metabolic markers (lipids, liver function, hematocrit). This tells you what’s actually driving your symptoms.
2. A clear understanding of your goals. Are you trying to preserve fertility? Maximize muscle gain? Restore sexual function? Recover from years of fatigue? Your goals matter because they directly influence which treatment makes sense.
3. A comparison of mechanisms. Enclomiphene and TRT do fundamentally different things to your body. You need to understand those differences, not just hear “both raise testosterone.”
4. Individual health context. Your age, prior medical history, family history, existing medications, and lifestyle all influence whether one treatment is safer or more effective for you.
5. A monitoring protocol. You don’t start and disappear. You get follow-up labs at 6 weeks, 12 weeks, and beyond to confirm you’re responding, adjusting dose as needed, and catching side effects early.
Importantly, this is what MOPE Clinic does on day one. It’s also what most other providers skip.
The MOPE Clinic Solution
At MOPE Clinic in Metairie and serving New Orleans and the greater South Louisiana region, we make this comparison straightforward:
Step 1: Full Lab Panel Before any prescription, you get comprehensive labs. We’re not guessing at your testosterone level—we’re measuring free testosterone, bound testosterone, estradiol, LH, FSH, SHBG, and metabolic markers. We’re looking at the full picture of why you feel the way you do.
Step 2: Education & Comparison You’ll sit down with our providers and discuss exactly how enclomiphene and TRT differ, which one aligns with your fertility plans, your lifestyle, your goals, and your health history. No sales pitch. No assumptions.
Step 3: Personalized Prescription If you’re a candidate for either treatment, we’ll outline which we recommend and why. You’ll understand the dosing, the monitoring schedule, the expected timeline, and what to watch for.
Step 4: Ongoing Lab Monitoring You don’t disappear after day one. We recheck labs at 6 weeks, adjust dose as needed, and continue monitoring. If side effects emerge, we catch them early. If you’re not responding, we adjust or pivot.
This is the standard of care. It’s also rare. And it’s why MOPE Clinic is LegitScript certified.
The Science: Enclomiphene vs TRT—A Direct Comparison
Now, let’s get specific. What actually is each treatment, and how do they differ?
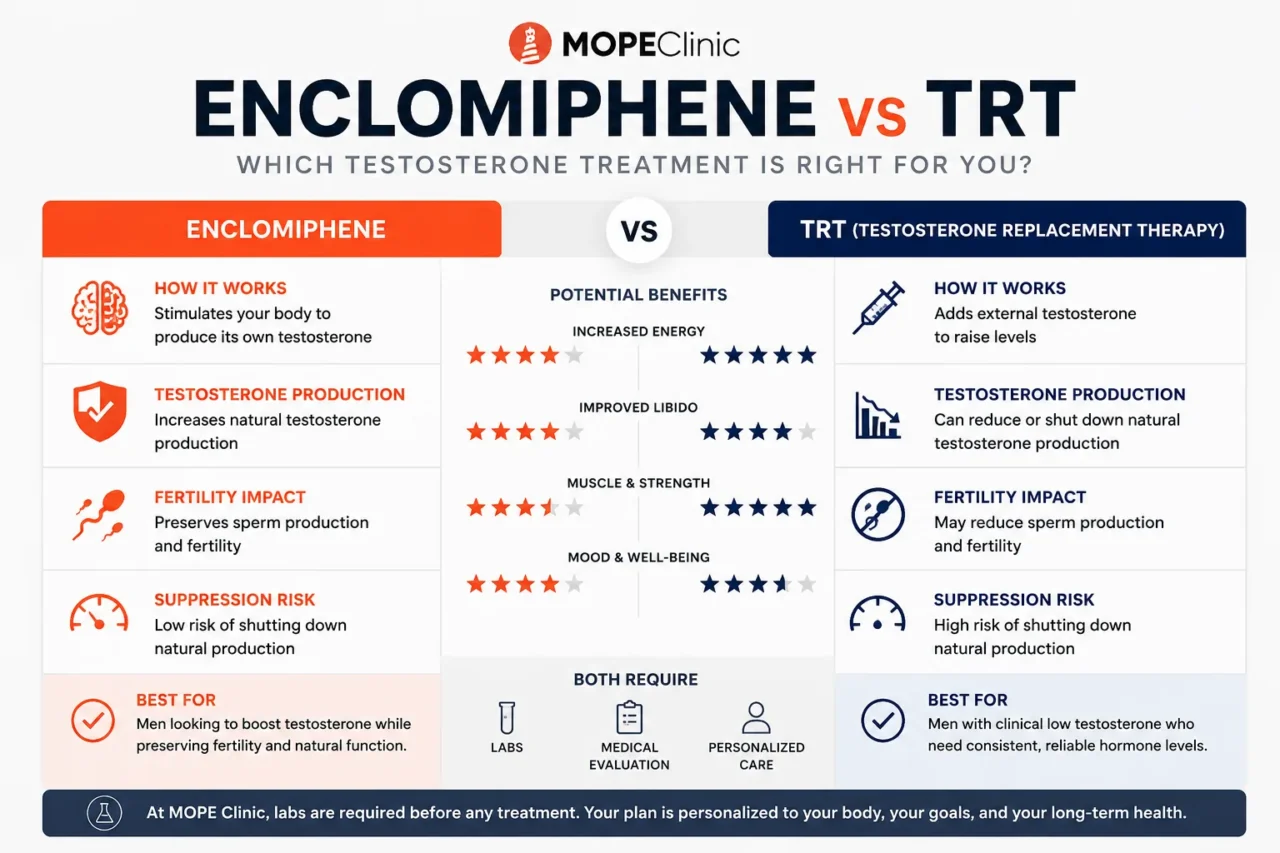
How Enclomiphene Works
Enclomiphene is the active enantiomer (half) of clomiphene citrate. It’s a selective estrogen receptor modulator (SERM) that works by blocking negative feedback in your brain.
Here’s the pathway:
- Normally, when testosterone is high, your brain senses this and reduces LH (luteinizing hormone) production—a feedback loop.
- Enclomiphene blocks this feedback at the pituitary level, telling your body: “Make more LH.”
- Higher LH signals your testicles to produce more testosterone—naturally.
- Your testicles stay functional and active.
As a result, testosterone rises because your body is making it, not because you’re receiving it externally.
How TRT Works
Testosterone replacement therapy (usually given as injections, gels, or pellets) works by adding external testosterone directly.
Here’s the pathway:
- You inject or apply testosterone.
- Your testosterone level rises.
- Your body senses the high level and reduces LH production—the opposite of enclomiphene.
- Your testicles downregulate and stop producing testosterone naturally.
- You’re now dependent on external testosterone to maintain levels.
In contrast, testosterone rises because you’re receiving it externally, not because your body is producing it.
Enclomiphene Pros and Cons
1. Preserves Natural Testosterone Production Your testicles keep working. If you stop treatment, your body can resume natural production (though recovery can take weeks to months). This is huge for men who might want biological children later.
2. Preserves Fertility Since your testicles stay active, sperm production continues. Men on TRT often experience azoospermia (no sperm) because testosterone suppresses FSH, which is needed for sperm production. Enclomiphene, by contrast, elevates FSH naturally.
3. Lower Risk of Testicular Atrophy Your testicles continue to be stimulated by LH and FSH, so they maintain size and function.
4. Potentially Lower Long-Term Cost If your dose is optimized, you may need lower total testosterone to maintain functional levels since you’re stimulating endogenous production.
5. Feels More “Natural” to Some Men Your body is making the testosterone, not receiving it. Psychologically, this matters to some patients.
Enclomiphene – Cons
1. Less Predictable Dosing Enclomiphene stimulates your body’s own production, but individual response varies widely. Some men are highly responsive; others need higher doses. This means more frequent lab adjustments.
2. Requires Understanding of LH/FSH Dynamics To monitor enclomiphene properly, you need repeat labs checking LH, FSH, and testosterone. Providers who don’t understand this mechanism will miss problems.
3. Side Effects Can Be Subtle Estrogen can rise as a side effect of higher testosterone production. If not monitored, men can develop gynecomastia (breast tissue growth), water retention, or mood changes. This requires active lab monitoring and sometimes additional medications (like aromatase inhibitors).
4. Slower Onset It takes time for LH to rise, then for testicles to respond, then for testosterone to climb. Full effects may take 4-12 weeks. Men looking for faster results may get impatient.
5. May Not Raise Testosterone Enough In men with primary hypogonadism (testicles that don’t work well), enclomiphene may not raise testosterone sufficiently because the testicles themselves are the limiting factor.
6. Not All Labs Measure It Accurately Enclomiphene is newer, and some standard labs don’t test for it accurately. You need specialized testing.
TRT Pros and Cons
1. Highly Predictable Dosing Inject 50mg testosterone weekly, and you know roughly what your level will be. The dose-response is much more linear and predictable than enclomiphene.
2. Faster Results Testosterone levels rise quickly—often within 1-2 weeks of starting injections.
3. Easier Monitoring You’re just checking testosterone level, maybe estradiol. Most labs can do this standard test. No exotic hormone panels required.
4. Works in Most Men Even men with primary hypogonadism (testicles that don’t produce testosterone well) respond to TRT because you’re adding testosterone directly.
5. Dosing is Flexible You can adjust dose up or down based on response, labs, and goals. More control.
6. Long-Established Safety Profile TRT has been used for decades. We have long-term data on cardiovascular effects, cancer risk, and other outcomes. (Note: this data is mixed and requires ongoing monitoring.)
TRT – Cons
1. Permanently Suppresses Natural Production (Short-Term) Once you start TRT, your body stops making testosterone naturally. If you stop treatment, recovery takes weeks to months—and is not guaranteed.
2. Kills Sperm Production TRT suppresses FSH and LH, which shut down sperm production. Men on TRT often have zero sperm count (azoospermia). If you want biological children, you need to plan this carefully or use fertility preservation strategies before starting.
3. Causes Testicular Atrophy Without LH stimulation, testicles shrink. This is usually reversible if you stop, but it’s psychologically concerning for many men and takes time to recover.
4. Higher Estrogen Conversion More testosterone = more aromatization to estradiol. Men on TRT often need aromatase inhibitors to prevent gynecomastia, water retention, and mood issues. This adds complexity.
5. Requires Lifelong Commitment Once you start, most men stay on TRT indefinitely. This is often the right choice, however it’s a long-term medical commitment.
6. Cardiovascular and Hematologic Risks TRT can increase red blood cell count (polycythemia), which may increase clot risk. Testosterone’s effects on cardiovascular health are debated—some studies show benefit, others show risk. This additionally requires ongoing monitoring, especially in men with existing cardiac risk.
7. Increased Prostate Specific Antigen (PSA) TRT can raise PSA levels, requiring closer prostate cancer screening. Men with a family history of prostate cancer need careful consideration.
8. Dependency You’re dependent on external testosterone. If you miss injections or can’t access your medication, testosterone crashes quickly.
Key Differences Between Enclomiphene and TRT
| Factor | Enclomiphene | TRT |
|---|---|---|
| Natural Production | Preserved | Suppressed |
| Fertility | Preserved | Often compromised |
| Testicular Function | Maintained | Atrophied |
| Speed of Effect | Slower (4-12 weeks) | Faster (1-2 weeks) |
| Predictability | Variable | Highly predictable |
| Monitoring Complexity | Higher (LH, FSH, T) | Lower (mainly T, E2) |
| Side Effect Profile | Estrogen-related | Estrogen + cardiovascular + hematologic |
| Long-Term Dependency | No (usually) | Yes |
| Cost | Potentially lower | Higher (lifelong) |
| Evidence Base | Emerging (newer) | Decades of data |
| Best For | Younger men, fertility concerns, hypogonadism due to secondary causes | Older men, primary hypogonadism, men not concerned about fertility |
Why MOPE Clinic’s Lab-Based Approach Matters in South Louisiana
Why Louisiana Lifestyle Matters
Living in Metairie, New Orleans, or anywhere in South Louisiana means you’re navigating heat, humidity, and a lifestyle that affects testosterone levels. Our sweltering summers can dehydrate you, stress hormones stay elevated in stressful periods, and the local diet—rich and sodium-heavy—influences your baseline metabolic health.
This is precisely why a “standard dose” doesn’t work.
A 35-year-old man in New Orleans dealing with heat stress and a high-pressure job has different testosterone needs than a 45-year-old retiree in Slidell. Additionally, a 50-year-old in Houma with metabolic syndrome needs a completely different treatment plan than a 50-year-old in Mandeville with no other health issues.
Why Personalized Labs Matter
MOPE Clinic’s comprehensive baseline labs account for your South Louisiana context: your actual metabolic health, your stress markers, your hematocrit (important because our heat and activity levels affect red blood cells), and your individual testosterone baseline.
Then we choose: enclomiphene or TRT—not because one is universally “better,” but because it’s better for you.
Internal Link Block
Related MOPE Clinic Articles:
- The Relationship Between DHEA and DHT: Understanding Hormone Interactions
- Testosterone Replacement Therapy (TRT): A Comprehensive Guide
- Good Candidate for Testosterone Therapy: How to Know if TRT is Right for You
- Clomiphene, Enclomiphene & Testosterone Optimization
- Stress, Cortisol, and Testosterone: The Weight Loss Connection
External Link Block
External Resources for Further Learning:
- National Library of Medicine: Testosterone Replacement Therapy in Hypogonadism
- Mayo Clinic: Testosterone Therapy: Benefits and Risks
- Endocrine Society Clinical Guidelines: Testosterone Replacement Therapy in Adult Males
- PubMed Central: Enclomiphene vs. Exogenous Testosterone
FAQ Section
Q: If enclomiphene preserves fertility, why would anyone choose TRT?
A: Because not everyone cares about fertility. Men over 60, men who have already had children and are done with family planning, or men with severe primary hypogonadism (where enclomiphene won’t work) often benefit more from TRT. However, TRT also works faster and tends to be more predictable. The choice depends on your individual situation, not on which one is objectively “better.”
Q: Can I switch from TRT back to enclomiphene?
A: Potentially, but it’s complicated. If you’ve been on TRT for months or years, your body’s natural testosterone production has downregulated significantly because of doing that. Stopping TRT and starting enclomiphene requires careful monitoring—you need to give your testicles time to wake up again, which can take 3-6 months. It’s possible but requires expertise and patience. This is another reason why choosing the right treatment from the start matters.
Q: How do I know if I actually have low testosterone?
A: This is the critical question most men skip. Many symptoms attributed to “low testosterone”—fatigue, low mood, reduced motivation—are actually caused by poor sleep, stress, diet, or lack of exercise. A real diagnosis requires labs. MOPE Clinic measures comprehensive hormone levels plus metabolic markers to ensure testosterone is actually the problem before treating it.
Q: What if I try enclomiphene and it doesn’t work?
A: Then you pivot. Some men don’t respond adequately to enclomiphene (especially if they have primary testicular failure), and TRT becomes the right choice. This is why starting with full labs and an expert team matters—you’ll know relatively quickly if it’s working, and you can adjust.
Q: Do I need an aromatase inhibitor with either treatment?
A: Possibly. With TRT, estrogen conversion is often high enough to warrant an AI in many men. With enclomiphene, if your testosterone and estradiol rise together appropriately, you might not need one. But some men do. This is determined by your individual lab response and requires monitoring.
Q: Is one treatment safer than the other?
A: Different, not safer. TRT has more cardiovascular and hematologic concerns. Enclomiphene has more estrogen-related concerns and variable response. Both, when monitored properly, are safe. When not monitored, both can cause problems. Therefore lab-based medicine matters.
Q: How long does it take to feel results?
A: Enclomiphene: 4-12 weeks, sometimes longer. TRT: 2-4 weeks for some effects (mood, energy, libido), 8-12 weeks for muscle gain. But individual variation is huge. This is why realistic expectations matter.
Q: Can I take supplements instead?
A: Supplement testosterone (DHEA, tribulus, etc.) doesn’t work for actual low testosterone. These are marketing products, not medicine. If your testosterone is clinically low, you need a real treatment prescribed by a real doctor. This is why MOPE Clinic is LegitScript certified—we don’t cut corners.
Ready to Find Out Which Treatment is Right for You?
Stop guessing. Get your comprehensive hormone panel, sit down with an expert who can explain enclomiphene and TRT in the context of your individual situation, and make a decision based on science—not internet advice or hype.
Call MOPE Clinic at 504-265-5491 to schedule your consultation. We serve Metairie, New Orleans, and throughout South Louisiana.
Or take our hormone health quiz to get a personalized sense of whether hormone optimization might be right for you.
MOPE Clinic: Real medicine. Real labs. Real results.